
Urology Disposable Products
MEDEREN provides high quality urological and endourological disposables manufactured with ISO 13485:2003 and CE 1023 standards. All our equipment is designed to perfection and can perfectly meets the needs of urology, diagnostic and therapeutic procedures.


Silicone Coated Latex Foley Catheters
- 2-way or 3-way 6-30 Fr/Ch
- Standard 400 mm
- Female 230 mm
- Pediatric 270 mm


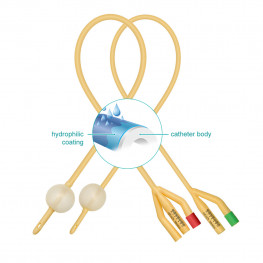
Latex Foley Catheters with Hydrophilic coating
- 2-way or 3-way 6-30 Fr/Ch
- Standard 400 mm
- Female 230 mm
- Pediatric 270 mm
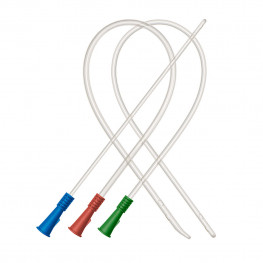
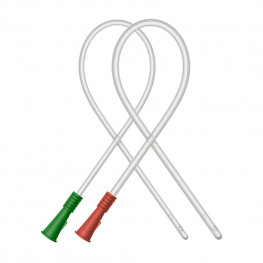
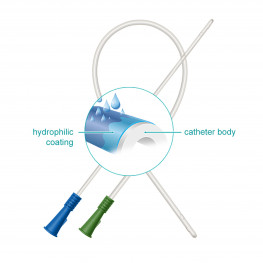
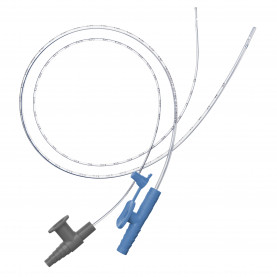
PVC Nelaton Catheters
- Standard: 400 mm, Fr 12-24
- Tiemann tip: 400 mm, Fr 6-24
- Female: 180 mm, Fr 6-24
- Pediatric: 400 mm, Fr 6-10
















MEDEREN provides genuine endo urological disposables like foley, nelatone, uretric catheters, urinebags and holders, uretrial stents etc. All the endourological disposables manufactured & as per ISO 13485 : 2003 and CE 1023 standards.
Urinary catheterisation should not be undertaken lightly and should be avoided wherever possible: it is painful (rated above lumbar puncture and arterial blood gases).It may also cause significant morbidity and even mortality. However, it is a procedure that is frequently necessary and unavoidable.
Nurses undertake the majority of catheterisation in primary care but GPs may be called upon to undertake it at times and then the doctor needs to be confident and competent. Sometimes difficulty can occur inserting a catheter, especially if there are problems such as urethral stricture, carcinoma of the prostate or following trauma. In such cases, rather than persevering, it is more judicious to seek help from someone with greater urological experience. As ever, act within your competency: the uninitiated should not use introducers and suprapubic catheterisation is also best left to the more experienced practitioner.
Indications
Be clear from the outset as to the aim of catheterisation.
Short-term indications include:
- Treatment of acute urinary retention.
- Pre-operative prophylactic emptying of the bladder prior to urological or pelvic surgery - eg, hysterectomy, caesarean section.
- Monitoring urine output in critically ill patients.
- Checking urinary residual volumes.
Long-term indications include:
- Treatment of chronic urinary retention due to bladder outlet obstruction not amenable to other treatment or those with neuropathic bladder.
- Management of incontinence:
- Intractable skin breakdown exacerbated by incontinence.
- The terminally ill or very frail where repeated bedding and clothing changes would be distressing.
- Patient preference after failure of other specific continence interventions.
Choice of catheter
Selection of the type of catheter should be based upon clinical need, anticipated duration of use, patient preference and risk of infection. Choices include:
- External versus indwelling catheters:
- Condom or penile sheath catheters can be an option in incontinent men without urinary retention but with severely impaired function and are particularly suitable for night-time use only.
- They are typically more comfortable and with lower rates of bacteraemia than indwelling catheters but are prone to leakage; risks include skin breakdown, urethral diverticulae and penile ischaemia.
- Intermittent catheterisation (IC) versus indwelling catheters:
- Intermittent self-catheterisation is preferable to chronic indwelling catheterisation in many with a neuropathic bladder: it provides freedom from urinary collection systems. It is the standard of care in those with spinal cord injuries. However, it may not be acceptable or feasible functionally for some patients.
- If used following surgery (eg, post-hysterectomy or repair of hip fracture), IC appears to be associated with reduced levels of bacteraemia and a quicker return to normal voiding. Used in the longer term, it appears to be associated with bacteriuria but less frequent UTI and less severe UTI than indwelling catheterisation.
- IC and indwelling catheters are not mutually exclusive and many combine both methods to accommodate individual needs and lifestyles.
- Urethral versus suprapubic catheters (SPCs):
- SPCs offer advantages such as comfort and more convenient catheter changes; they can be clamped to test voiding and may offer better self-image and sexual function.
- Disadvantages include risk of cellulitis, leakage, and prolapse through the urethra; higher levels of expertise are required for insertion.
Catheters come in a large variety of sizes, materials (latex, silicone, Teflon®) and types (Foley catheter, straight catheter, Coudé tip catheter).
Types
Self-retaining Foley catheters are perhaps the best known and are soft plastic or rubber tubes inserted into the bladder to drain urine, held in place by a balloon at the tip of the tube, inflated with sterile water.
Materials
- The original Foley catheters were made of latex rubber but this has become obsolete. Latex is flexible and cheap but is prone to infection and hypersensitivity reactions.
- Silicone latex Foley catheters are very similar but have a silicone layer on top of the latex to overcome the endothelial irritation and microscopic lacerations/stricture development associated with latex. Some patients are allergic to latex. The silicone layer tends to become damaged after a while and the underlying latex may again come into contact with the urothelium, which restricts the use of silicone latex catheters to 1-2 weeks when they should either be removed or replaced. Hydrogel is an alternative latex coating.
- Silicone Foley catheters (where all latex is replaced by silicone) are 5-10 times as expensive as the silicone latex but their relative price has fallen as they have become more popular. As well as having a longer life of 6-8 weeks (some manufacturers claim up to three months), they are more rigid which can be advantageous. The balloon tends to empty by loss of water due to a semi-membranous effect of the wall of the balloon and so it will need to be refilled periodically. With longer life, encrustations tend to form at the tip of the catheter which may narrow the orifice or increase the diameter of the catheter, causing pain and bleeding upon removal. Therefore, they should not be left beyond the recommended limit.
- Coating catheters with materials with antimicrobial properties has been tried to prevent biofilm and encrustation related problems.Methods include use of:
- Silver alloys (so-called 'silver catheters').
- Antibiotic-coated or electrified catheters.
The indication will influence the choice of catheter:
- For simple pre-operative catheterisation or in hospitalised patients requiring short-term catheterisation only, a silver catheter may be preferred. There is evidence that this reduces the risk of catheter-acquired UTI but overall cost-effectiveness has not been confirmed.
- If the bladder is to be emptied and/or a urinary specimen taken with no need for ongoing catheterisation, a straight catheter (also known as a Nelaton catheter) is used and immediately discarded. This has no facility for retention and tends to be made of PVC with a large lumen to facilitate rapid urine flow.
- If the catheter is to be left in situ, an indwelling Foley catheter is used. A silicone Foley catheter has a much longer life than a latex-silicone one, so tends to be preferred for longer-term use, although a Cochrane review concludes there is insufficient comparative evidence to be able to make good decisions between catheters for this type of use.
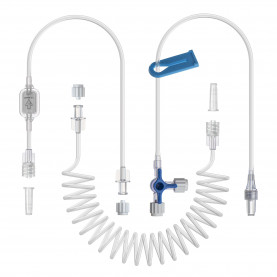
- Triple lumen catheters are commonly used for continuous bladder irrigation following bladder or prostate surgery.
- Catheters come with various tips. The standard straight is suitable for most occasions. Beware of types such as the Tiemann or Coudé tip with a curved tip designed to facilitate passage through the prostate. It is easy to produce false passages and to do much damage. The Whistle-tipped catheter has openings laterally and above the balloon to drain debris and blood clots.
Sizing
- Foley catheters are sized in Charrieres, also known as French Grade (FG): 1 Ch = 1/3 mm diameter. Selection of the right catheter size should increase patient comfort and allow adequate drainage (a 12 Ch catheter has a drainage capacity of 100 litres in 24 hours).
- The smallest size of catheter allowing effective drainage should be used, as larger gauges are more likely to cause trauma and mucosal irritation. However, where there is infection or postoperative bleeding, a larger bore minimises the risk of obstruction.
- The following provides an approximate guide to which size of catheter to insert in specific circumstances:
- Initial catherisation (female), with clear urine, containing no grit (encrustation), debris or haematuria - 10-12 Ch/3.3 mm.
- Initial catheterisation (male), with clear urine, containing no grit, debris or haematuria - 12-14 Ch/4 mm.
- Initial catheterisation (male) with clear or slightly cloudy urine, no or mild grit, light haematuria with no or small blood clots only - 16 Ch/5.3 mm.
- Initial catheterisation (male) with moderate-to-heavy grit or debris, haematuria with moderate clots - 18 Ch/6 mm*.
- Very cloudy urine with heavy grit and debris, haematuria with moderate-to-heavy blood clots (usually used postoperatively following bladder/prostatic surgery) - 20 Ch/6.7 mm*.
- Following bladder/prostatic surgery or trauma with severe haematuria containing large blood clots - 22 Ch/7.3 mm*.
- Smaller sizes are suitable for children.
- If a catheter is being replaced, note the size of the one to be removed.
- Catheters can be prescribed on FP10s; specify 'male' or 'female', as this will determine length.
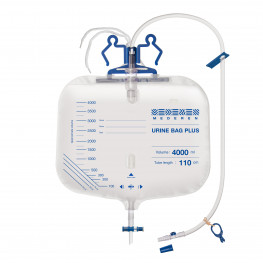
Drainage systems
- There is a wide range of drainage systems available and choice will depend on method of catheterisation and the individual's needs.
- Most common is the urinary drainage bag - these can be attached to the leg (at the thigh, knee or calf) and have different capacities (usual for adult - 350-750 ml). Body-worn bags are intended for daytime use to enable mobility, whilst larger-capacity bags are used for night-time drainage. Night bags sometimes have a drainage tap to facilitate emptying and can remain in situ for up to 5-7 days. They should be used with a hanger, either on the bed or free-standing.
- It is important to maintain a 'closed drainage system' (ie connecting the catheter and drainage bag as a continuous unit) to reduce the risk of UTIs.
Technique
Catheterisation should always be an aseptic, 'no-touch' technique. A 'no-touch' technique reduces the risk of introducing infection into the bladder. Touch only the plastic packaging that contains the catheter, and not the catheter.
Equipment
Before starting, check that all the necessary equipment is present:
- Sterile gloves.
- Suitable antiseptic.
- Swabs or cotton wool.
- Sterile paper towels.
- Antiseptic, anaesthetic lubricating gel.
- Appropriate range of catheters.
- Receptacle for urine or, if the catheter is to be left in situ, a urine bag with tube to connect to the catheter.
- If a Foley catheter is to be used, a syringe of appropriate size and water or saline for the bulb
Male catheterisation
With the patient supine:
- Use the nondominant hand to hold the penis - this hand is the non-sterile hand and holds the penis throughout the procedure. Retract the prepuce (where uncircumcised and no phimosis).
- Clean the glans.
- With index finger and thumb behind the the glans, stretch the penis straight and slightly upwards to overcome the first curve of the urethra.
- Insert a few ml of gel (eg, lidocaine 2%) into the urethra, using the single-use insertion device, and allow some to spill over on to the surrounding glans to lubricate the catheter's insertion as well as anaesthetise the procedure. Allow some time (2-3 minutes) for the anaesthetic gel to take effect.
- To avoid urine spill, some connect a collecting bag to the catheter prior to the procedure whilst others use a small collecting bowl and, once flow starts, they kink the tube to obstruct it and then connect the bag.
- Allow the catheter to slip into the urethra until soft resistance is encountered - the second urethral curve. To overcome this, straighten the stretched penis, while pushing gently against the catheter. Sometimes, the penis needs to be turned further downwards, towards the bed, to enable passage of the catheter through the prostate.
- Once urine flow is achieved, push the catheter in as far as it will go or until the 'fork' of the catheter. This is to prevent the balloon from being inflated whilst still in the prostate.
- Inflate the balloon with the appropriate amount of water or saline (usually 10-15 ml). Retract the catheter gently until there is a slight tug to indicate that the balloon is resting in the correct position against the bladder neck or prostate. Urine should flow freely. Always replace the prepuce - failure to do so will cause a paraphimosis.
- Taping the tube to the inner thigh prevents any tug on the tube pulling on the catheter in the bladder.
Female catheterisation
As with male catheterisation; however, anatomically the female urethra is much shorter and without the obstacle of the prostate. Identifying the urethral orifice can sometimes be difficult. Again with the patient in the supine position:
- Wipe the area around the urethra with antiseptic.
- Lubricate the catheter tip with gel. Some advocate anaesthetising the urethra in advance of catheterisation. Open the labia and allow the catheter to slide inside.
- Where the urethral opening is not visible, try to palpate for it at the anterior side of the vagina where it can often be felt as a small horseshoe-like ridge. Using the index finger, guide the tip of the catheter into the opening.
- Push the catheter approximately 10 cm into the bladder to ensure that it is truly in.
- Fill a Foley catheter's balloon with the appropriate amount of water or saline. Then retract the catheter until there is a slight tug to indicate that the balloon now is in position against the bladder neck. Most of the catheter tube usually protrudes from the urethra.
Insertion problems
Include:
- Phimosis (men only) - where the opening is adequate, try to pass the catheter blind. If the opening is too narrow, try dilating it with sounds or a smaller catheter. If in doubt, seek more expert help.
- Failing to pass the prostate (men only) - try a catheter with a larger diameter. Prostatic urethra is not narrow but squashed flat by the surrounding prostate. A larger catheter overcomes this distortion and allows passage. Another option is to try a silicone catheter, as it is more rigid than a silicone latex catheter.
- Failing to pass the bladder neck - try a smaller size.
- False passage, especially if catheterisation is traumatic. Never push past resistance during insertion.
- Urinary retention where the lumen of the catheter has become blocked after using too small a catheter. A catheter with an overly small diameter will allow the catheter to move, bulge and slide within the urethra, causing short-term irritation, but chronically may lead to stricture formation.
Catheter management problems
These commonly include:
- Leaks - exclude constipation, bladder spasm and catheter blockage. Use a smaller-gauge catheter.
- Encrustation is due to the precipitation of minerals and other material (eg, mucus, protein and bacteria) on to the catheter and is a common occurrence (causing recurrent blockage in 40-50% of long-term catheterised patients), exacerbated by Proteus spp. infection and alkaline urinary pH. Increasing fluid intake, acidification of urine (instilled solutions, vitamin C, cranberry juice), treating infection, use of larger-bore catheters and irrigation solutions may help.
- Inflammation - foreign body reaction, exacerbated by infection and encrustation. Try a different type of catheter.
- Bladder spasm - intermittent clamping of catheters, gradually lengthening the time clamped or the use of catheter valves, may help the bladder to retain/maintain its capacity and tone. Antispasmodics (eg, oxybutynin) may be effective at providing relief from spasm.
- Blockage requires catheter change. Try to establish if a pattern of blockage can be established, usually towards the end of the lifespan of a catheter, and move to more regular changes.
Removing a catheter
- Timing - traditionally an indwelling catheter is removed early in the morning so that if micturition does not follow, this will become apparent during daytime hours, allowing recatheterisation. A valid alternative is to remove it just before the patient goes to sleep at night. It is usual to empty the bladder before retiring and to sleep through the night and it is only if a full bladder cannot be emptied in the morning that the catheter is replaced. What is important is to choose a time so that, if voluntary micturition does not occur, timely reaction will occur without the disruption of anyone's sleep.
- When the time comes to remove the catheter, attach a syringe to the orifice to the balloon and draw back on the plunger to suck out the water or saline in the balloon and then gently pull the catheter out.
- If the balloon will not empty:
- Try being more gentle with traction on the plunger of the syringe, as excessive pressure may have collapsed the tube so that water will not flow.
- Try instilling another 1 or 2 ml of water to unblock any adhesions.
- Try wiggling and rotating the catheter whilst pulling the plunger.
- Cut the catheter a little way outside the urethra. Be careful that the catheter does not retract and disappear into the bladder. It may be necessary to insert a safety pin through it to prevent this and leave the catheter for an hour or two whilst the balloon slowly empties.
- If the balloon remains rigid, it may be possible to locate and puncture it by digital examination and use of a prostatic biopsy needle. This is done through the rectum in men and the vagina in women.
- It may be possible to over-inflate the balloon and burst it. If this is done it should be followed by cystoscopy to ascertain that no pieces are left in the bladder.
New products
All products



















Latest news
All posts
Better Infusion Pump choise for 5-FU
Because of its long infusion time over 46–48 hours, 5-fluorouracil (5-FU) is usually administered with an ambulatory infusion pump in the outpatient setting. However, two types of pumps...
Belfast Team Invents Self-sterilizing Antiviral Disposable Materials
It’s early days before your doctor’s clothes will be self-sterilizing from the patient before you, but the cheap-to-produce film could still be a game-changer
Meet us at these shows and exhibitions in 2023
We love meeting you face to face, catching up with your business developments, and showing you what new products we have to offer.

Happy Holidays! Shana Tova!
Thank you all for your trust and continued work to improve patient and caregiver safety with us.
Zebra Medical Vision Secures FDA Nod For Device That Identifies Water In The Lungs
Zebra Medical Vision, the AI medical imaging insights company, announced Wednesday it has received its fourth FDA 510(k) clearance for the HealthCXR device intended for the identification...

World’s first robot-assisted brain aneurysm surgery performed in Toronto
TORONTO – A team of Toronto doctors has completed the world’s first brain aneurysm surgery using robotics, leading to hope of better treatment for aneurysm and stroke patients,...